
View resources
Key points
- Transient synovitis is a benign condition and the most common cause of an acute limp in children.
- Careful assessment (history and examination) can identify red flags suggestive of more serious pathology (which require investigation and specialist referral).
- Septic arthritis is an orthopaedic emergency and should be suspected in any limping child with severe, localised joint pain and fever.
Purpose
This document provides clinical guidance for all staff involved in the care and management of a child presenting to an Emergency Department (ED) with an unexplained limp in Queensland. This guideline does not cover the management of all conditions that can present with limp but focuses on identifying the more common serious conditions (including septic arthritis) that require timely specialist referral.
This guideline has been developed by senior ED clinicians across Queensland, with input from Orthopaedic and Rheumatology specialists, Queensland Children’s Hospital, Brisbane. It has been endorsed for use across Queensland by the Queensland Emergency Care of Children Working Group in partnership with the Queensland Emergency Department Strategic Advisory Panel and the Healthcare Improvement Unit, Clinical Excellence Queensland.
Introduction
Children present to the ED with a wide spectrum of possible causes for a limp ranging from benign conditions to serious underlying pathology. Common conditions are discussed within this guideline, including an approach to initial assessment and management. A broader range of conditions may need to be considered, especially if the limp has persisted for more than one week.
Broader range of diagnostic differentials for acute and persistent limp
| Category | Conditions |
|---|---|
| Infection |
|
| Post-infection |
|
| Trauma (accidental or non-accidental) |
|
| Primary bone disease |
|
| Referred pain |
|
| Other | Neoplastic, inflammatory, non-inflammatory (mechanical or anatomical) conditions, haemophilia (can be atraumatic), chronic pain syndrome or psychogenic disorders. |
Septic arthritis commonly occurs in children aged less than three years but can occur at any age.
Consider septic arthritis in any child with joint pain and fever.
Common causes of acute limp by age and order of incidence
| Frequency | Less than 1 year | 1- 4 years | 5 -10 years | Over 10 years |
|---|---|---|---|---|
Most common |
|
|
|
|
Common ED presentation
| Transient synovitis | |
|---|---|
| History |
|
| Examination |
|
| Diagnosis |
|
| Management |
|
Less common but serious ED presentations
| Septic arthritis | |
|---|---|
| History |
|
| Examination |
|
| Diagnosis |
|
| Management |
|
| Osteomyelitis | |
|---|---|
| History |
|
| Examination |
|
| Diagnosis |
|
| Management |
|
Perthes disease
- idiopathic avascular necrosis of the proximal femoral epiphysis
- 20% of cases are bilateral
- diagnosis may be delayed due to fluctuating symptoms and potential for normal X-ray in early stages

| Perthes disease | |
|---|---|
| History |
|
| Examination |
|
| Diagnosis |
|
| Management |
|
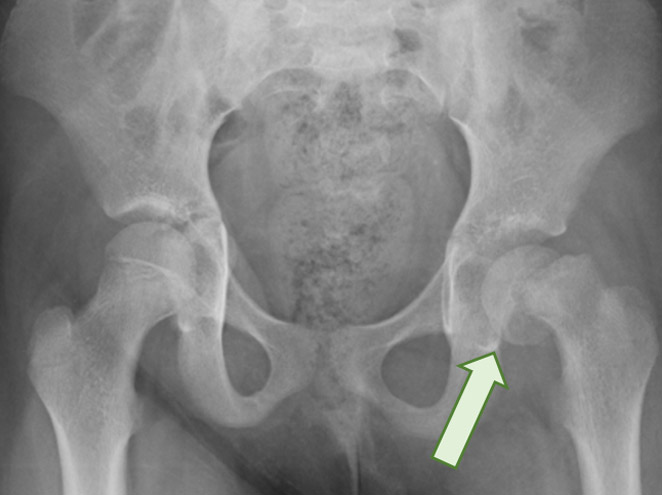
Slipped Upper Femoral Epiphysis (SUFE)
- greatest risk factor is weight greater than 90th percentile
- 20% of cases are bilateral4
- diagnosis may be delayed as symptoms may be subtle
- more common in children with endocrine disorders / disturbances (puberty)
- high risk of avascular necrosis
| Slipped upper femoral epiphysis (SUFE) | |
|---|---|
| History |
|
| Examination |
|
| Diagnosis |
|
| Management |
|
Assessment
The aim of the assessment is to differentiate the children who have serious underlying pathology from the larger group of children who do not have a serious cause for their limp.
History
History taking should include specific information on:
- onset and course of limp
- history of trauma
- pain history – including localisation, magnitude, pain migration, number of joints involved, exacerbating/ relieving factors
- constitutional symptoms such as fevers, malaise, anorexia, weight loss, night sweats
- bleeding history- excess bruising/bleeding, prolonged/frequent epistaxis, prolonged bleeding after invasive procedures
- preceding illness including sore throat or skin infections
- previous or recurrent injuries (haemophilia, or should raise suspicion of NAI especially in infants and younger children)
- social history
- developmental delay
Examination
Clinical examination should include:
- general examination with attention to vital signs and appearance, bruising and lymphadenopathy
- neurological examination – symmetry of limbs, muscle atrophy, power, tone, reflexes and coordination, including ataxia
- joint examination (including joint above and below) assessing swelling, tenderness, warmth, active and passive mobility
- point bony tenderness (may indicate osteomyelitis)
- abdomen, scrotum and spine examination to exclude referred pain from other possible causes
Considerations in children
- physical examination can be challenging in younger children – observation of how they move, weight bear, crawl, walk, run, jump and squat will be very helpful in terms of localising potential pathology
- neurological weakness can present as a limp.
Septic arthritis is an orthopaedic emergency. Delay in diagnosis increases the risk of joint destruction.
- fever greater than or equal to 38.5°C
- recent throat or skin infection
- inability to weight bear or severe, localised joint pain
- bony pain
- systemic symptoms such as weight loss, night sweats
- possible unwitnessed trauma/NAI
- overweight adolescent
Suspect septic arthritis in child with a fever greater than 38.5°C, acute onset of severe, localised joint pain and difficulty weight bearing.
Seek urgent senior emergency/orthopaedic advice as per local practice if septic arthritis is suspected.
Investigations
Investigations required will depend on the assessment. Children presenting within a few days of onset of the limp and with no red flags may not require any investigations. Clinicians must ascertain the benefits before ordering tests and clarify what a specific test will add to the evaluation of the limping child.
Investigations for a child with a limp
| Investigation type | Utility |
|---|---|
| Plain X-rays |
|
| Full blood count |
|
| C reactive protein |
|
| Erythrocyte sedimentation rate |
|
| Coagulation |
|
| ASOT/Anti DNase |
|
| ECG |
|
| Throat/wound swab M/C/S |
|
| Blood cultures |
|
| Joint ultrasound |
|
| Specialised imaging |
|
Diagnosing septic arthritis
Definitive diagnosis is confirmed on positive joint aspirate by orthopaedic surgeons in theatre. In the ED, Kocher’s criteria6-8 can assist in determining the likelihood of septic arthritis.
| Predictors | Probability of septic arthritis | |
|---|---|---|
| Number of predictors | Probability of septic arthritis |
| 0 | 0.2% | |
| 1 | 3% | |
| 2 | 40.0% | |
| 3 | 93.1% | |
| 4 | 99.6% | |
There is a modified Kocher which also uses a CRP of >20.
Management
Refer to the flowchart [PDF 486.63 KB] for a summary of the recommended assessment and investigation for a child presenting to ED with an unexplained limp.
The appropriate management will be guided by the outcome of the assessment.
Urgent referral to orthopaedic team as per local practice is required for all children with suspected septic arthritis.
If suspected septic arthritis and unwell or septic, give urgent empiric antibiotics after blood cultures obtained. Do not delay whilst waiting for operative intervention. This management should be as per statewide sepsis protocols.
Prompt referral to orthopaedic service as per local practice is required for all children with concerns of serious underlying pathology.
Consider seeking orthopaedic advice as per local practice for a child with a persistent limp (greater than one week) and a normal X-ray.
Escalation and advice outside of ED
Clinicians can contact the services below if escalation of care outside of senior clinicians within the ED is needed, as per local practices. Transfer is recommended if the child requires a higher level of care.
Septic arthritis is an orthopaedic emergency. Suspect in any limping child with severe, localised joint pain and fever.
Child with septic arthritis (requires time-critical care)
| Reason for contact | Who to contact |
|---|---|
| For urgent advice and referral of child with suspected septic arthritis | Contact the onsite/local orthopaedic service. The onsite/local paediatric service may assist with emergency management. |
Non-critical child
| May include children with |
|---|
|
| Reason for contact | Who to contact |
|---|---|
| Advice (including management, disposition or follow-up) |
Follow local practices. Options:
|
| Referral | First point of call is the onsite/local orthopaedic service |
Inter-hospital transfers
| Do I need a critical transfer? |
|
| Request a non-critical inter-hospital transfer |
|
| Non-critical transfer forms |
|
Disposition
When to consider discharge from ED
Most children who do not have serious underlying pathology can be managed supportively at home, with appropriate advice around when to represent for review at either their GP or the ED.
Parents should be advised to represent for medical review (GP or ED) if the child develops a fever or symptoms persist or worsen.
Follow-up
Recommended follow-up is based on the outcome of the assessment. Follow-up is not routinely required for children for whom no serious underlying pathology is suspected.
When to consider admission
As per advice for children requiring specialist referral.
Consider admission for any child who cannot weight bear and is no longer mobile.
Related documents
-
- Kastrissianakis K, Beattie TF. Transient synovitis of the hip: more evidence for a viral aetiology. European journal of emergency medicine: official journal of the European Society for Emergency Medicine.2010;17(5):270-3.
- Baskett A, Hosking J, Aickin R. Hip radiography for the investigation of nontraumatic, short duration hip pain presenting to a children’s emergency department. Pediatric emergency care. 2009;25(2):78-82.
- Fischer SU,Beattie TF.The Limping Child: epidemiology, assessment and outcome.Journal of Bone and Joint Surgery.1999;81:1029-34
- Clarke NMP, Kendrick T. Slipped capital femoral epiphysis. BMJ. 2009;339.
- Plumb J, Mallin M, Bolte RG. The role of ultrasound in the emergency department evaluation of the acutely painful pediatric hip. Pediatric emergency care. 2015;31(1):54-8
- Herman MJ, Martinek M. The limping child. Pediatrics in review/American Academy of Pediatrics. 2015;36(5):184-95
- Kocher MS,Mandiga R,Zurakowski D,Barnewolt C,Kasser JR.Validation of a Clinical Prediction Rule for the Differentiation Between Septic Arthritis and Transient Synovitis of the Hip in Children.The Journal of Bone & Joint Surgery.2004;86(8):1629-35
- Kocher MS ZD, Kasser JR. Differentiating between septic arthritis and transient synovitis of the hip in children: an evidence-based clinical prediction algorithm. J Bone Joint Surg Am. 1999;81(12):1662-70.
-
Document ID: CHQ-GDL-60007
Version number: 4.0
Supersedes: 3.0
Approval date: 08/12/2023
Effective date: 20/12/2023
Review date: 08/12/2026
Executive sponsor: Executive Director Medical Services
Author/custodian: Queensland Emergency Care Children Working Group
Applicable to: Queensland Health medical and nursing staff
Document source: Internal (QHEPS) + External
Authorisation: Executive Director Clinical Services
Keywords: Limp, septic arthritis, Perthes, SUFE, Toddler’s fracture, rheumatic fever, 00733, paediatric, emergency, guideline, children, CHQ-GDL-60007
Accreditation references: NSQHS Standards (1-8): 1, 8
-
This guideline is intended as a guide and provided for information purposes only. View full disclaimer.
Last updated: March 2024