
View resources
Key points
- Anaphylaxis is a rapidly evolving generalised multi-system allergic reaction to an allergen or trigger characterised by respiratory and/or cardiovascular features that can be fatal.
- Anaphylaxis is under-recognised as symptoms may have resolved prior to ED presentation.
- Adrenaline IM into the thigh is the first line treatment for anaphylaxis.
- Severe anaphylaxis is a challenging clinical scenario that requires the most skilled clinicians available and rapid escalation of life saving measures.
- Caregivers of a child who has suffered anaphylaxis must receive two Adrenaline autoinjectors along with education on use and an individualised action plan on discharge from ED.
- Adrenaline autoinjectors must be prescribed (and if possible dispensed) to all children who have suffered any allergic reaction (mild, moderate or severe) secondary to nut exposure as subsequent exposures may lead to more severe reactions (including anaphylaxis) and are less predictable compared to other foods.
Purpose
This document provides clinical guidance for all staff involved in the care and management of a child presenting to an Emergency Department (ED) in Queensland with symptoms suggestive of an acute allergic reaction or anaphylaxis.
This guideline has been developed by senior ED clinicians and Paediatricians across Queensland, with input from Immunologists, Queensland Children’s Hospital, Brisbane. It has been endorsed for use statewide by the Queensland Emergency Care of Children Working Group in partnership with the Queensland Emergency Department Strategic Advisory Panel and the Healthcare Improvement Unit, Clinical Excellence Queensland.
Introduction
An allergic reaction is an immunologically-mediated adverse reaction which occurs when a person’s immune system reacts to a substance (allergen) in the environment which would normally be innocuous. Allergens can enter the body via a number of different portals, including inhalation, ingestion, contact with skin and injection (parenteral medication or insect stings and bites).
Up to 40% of children in Australia and New Zealand are affected by allergic disorders at some time during their life, with 20% having current symptoms. Allergic diseases have approximately doubled in western countries over the last 25 years. The most common allergic conditions in children are food allergies, eczema, asthma and hayfever (allergic rhinitis).1
Most allergic reactions do not cause major problems, even though for many people they may be a source of extreme irritation and discomfort. A small number of people may experience a severe allergic reaction called anaphylaxis.
Anaphylaxis is an acute systemic allergic reaction in response to an allergen or trigger. It is caused by an IgE-mediated release of histamine, leukotrienes and prostaglandins from tissue mast cells and peripheral blood basophils.1,2 This reaction is multisystem in nature with systemic cardiovascular and/or respiratory symptoms and involvement of other systems such as the skin and gastrointestinal tract. Anaphylaxis may also be accompanied by signs of general allergic reaction.1,3 Urticaria / skin symptoms may be transient or subtle. Emergency departments tend to miss the diagnosis of anaphylaxis if the symptoms have resolved or if there is not a previous history of anaphylaxis.4
Non-immunologic anaphylaxis or ‘anaphylactoid’ reaction is an acute systemic reaction which is clinically identical to anaphylaxis. This occurs as a result of direct mast cell stimulation in response to a trigger and requires the same treatment.3,5
Food allergies are the most common cause of anaphylaxis in children. Common allergens include peanuts, tree nuts, wheat, sesame, egg, cow’s milk, fish, shellfish and on rare occasions spices, fruit and soy.5 Other causative agents include drugs, insects, latex, allergen therapy and, less commonly, exercise, cold and immunisations. In up to 30% of reactions, a cause cannot be identified.1
The prevalence of anaphylaxis in the paediatric population is estimated to be 1 in 1000.6 Admission rates for anaphylaxis are increasing in Australia with food allergies affecting 4 – 8% of children less than five years of age.1 Deaths from anaphylaxis are relatively rare but they are increasing in Australia with 324 deaths recorded between 1997 and 2013.7
Risk factors for fatal anaphylaxis include:1,8
- asthma
- delayed administration of adrenaline
- age (teenagers and adults are at higher risk)
- nut allergy
Assessment
Emergency care should always involve a rapid primary survey with evaluation of (and immediate management of concerns with) airway, breathing, circulation and disability (ABCD). Pre-hospital treatment with IM adrenaline (see dosing advice below) should be initiated if any clinical suspicion of anaphylaxis.
History
History taking should include specific information on allergic symptoms prior to hospital presentation with particular emphasis on cardiovascular or respiratory symptoms.
Once the patient is stabilised, the allergen trigger for the event should be identified (if possible).
Questioning should identify:
- all foods and medications consumed several hours before the reaction
- any possible stings or bites
- current medications such as beta-blockers (as may affect response to treatment)
- co-morbid diseases such as asthma (as can affect the severity of the reaction)
Examination
| Generalised allergic reaction | Anaphylaxis |
|---|---|
Characterised by:
AND/OR
AND
| Any acute onset illness with typical skin features (urticaria, erythema, flushing) plus involvement of at least one of the following:
OR Any acute onset of hypotension or bronchospasm or upper airway obstruction, where anaphylaxis is considered possible even in the absence of skin features (urticaria, erythema, flushing)OR Abdominal pain or repetitive vomiting after an insect sting or injected medication |
Source: The Australian Society of Clinical Immunology and Allergy1
Anaphylaxis requires ONLY ONE respiratory or cardiovascular component to make a diagnosis.
Differential diagnosis
| Clinical presentation | Differential diagnoses |
|---|---|
| Swelling of lips and tongue | Idiopathic or hereditary angioedema |
| Cardio-vascular compromise including hypotension | All forms of shock |
| Stridor, drooling or respiratory distress | Upper airway obstruction causes including foreign body, epiglottitis, and croup |
| Flushing of the face, headache, heart palpitations, itching, blurred vision, cramps and diarrhoea within minutes to an hour of consuming contaminated fish | Scombroid poisoning (histamine poisoning from fish) – easily confused as seafood is a common cause of anaphylaxis |
Investigations
Investigations are not routinely recommended. Histamine levels fall too rapidly to be clinically useful. Occasionally tryptase levels collected within three hours of symptom onset may be useful but should only be collected on advice from Immunologist/Allergist.
The use of other laboratory and radiological tests should be guided by patient co-morbidities and circumstances, including incidental trauma.9
Management
Refer to flowchart [PDF 370 KB] for a summary of the emergency management of children with an acute allergic reaction.
Some insect bites or stings can result in severe abdominal pain and vomiting. This represents a severe allergic reaction and should be managed as for anaphylaxis.
Anaphylaxis is often under-diagnosed due to the variable nature and duration of symptoms.
Given the potential for rapid deterioration administer Adrenaline IM immediately into the thigh if anaphylaxis is suspected.
Anaphylaxis
Initial management includes rapid triage and clinical assessment of the patient’s airway patency, breathing (ventilation and oxygenation) and circulation. Intervention and stabilisation should occur immediately. Continuous cardiac and oxygen saturation monitoring is recommended. Children with less severe generalised allergic symptoms may initially appear stable but have the potential for rapid deterioration.9
Adrenaline
- Adrenaline IM into the thigh is the recommended first-line treatment of anaphylaxis
- effective for all the symptoms and signs of anaphylaxis2
- associated with a decreased fatality rate if administered promptly10
Studies have demonstrated that peak plasma levels are achieved significantly faster after IM injection into the thigh compared with SC injection into the arm.11,12 1 in 10 patients will need more than one dose of adrenaline.19
Nebulised Adrenaline may help relieve upper airway obstruction and/or bronchospasm but should only be administered in addition to Adrenaline IM.
Adrenaline IV should be reserved for the following children:
- immediately life-threatening profound shock
- circulatory compromise and continuing to deteriorate after Adrenaline IM
- refractory stridor or bronchospasm
- rebound of anaphylaxis despite recurrent more than 2 doses Adrenaline IM
Where Adrenaline IV is indicated, a continuous low dose Adrenaline infusion is the safest and most effective form of administration.13 Significant adverse events including fatal cardiac arrhythmia and cardiac infarction have been reported when Adrenaline IV is administered too rapidly, inadequately diluted or in excessive dose.14 An Adrenaline IV bolus can be considered for use in the hemodynamically unstable patient while preparing an adrenaline infusion.1 Staff with specialist training/most senior staff available will be required.
| Adrenaline dosing for the treatment of anaphylaxis in children | |
|---|---|
| Adrenaline (IM) | See dose banding table below (Dose recommendations have changed) See skill sheet for drawing up Adrenaline in anaphylaxis |
| Adrenaline (IV infusion) | With Smart Pump Drug Errors Reducing System: Without Smart Pump Drug Errors Reducing System: |
| Adrenaline (IV push dose) | 1 microgram/kg Take 1 mL of 1:10,000 adrenaline ampoule and make it up to 10 mL with 9 ml of sodium chloride 0.9% Final volume: 10 mL syringe: each 1 mL contains 10 micrograms of adrenaline (10 microgram/mL) Volume to administer: 0.1mL of this solution/kg see CREDD dosing See skill sheet for Adrenaline use in shock |
| IM Adrenaline dose banding (these doses are as per CREDD 2024) | |
|---|---|
| Indicative age | Dose and Volume of adrenaline 1:1,000 to administer |
| <10kg | 100 microgram (0.1 mL of 1:1,000) |
| 10-12kg | 100 microgram (0.1 mL of 1:1,000) |
| 13-15kg | 150 microgram (0.15 mL of 1:1,000) |
| 16-21kg | 200 microgram (0.2 mL of 1:1,000) |
| 22-34kg | 300 microgram (0.3 mL of 1:1,000) |
| 35-49kg | 400 microgram (0.4 mL of 1:1,000) |
| more than 50kg | 500 microgram (0.5 mL of 1:1,000) |
Seek urgent paediatric critical care advice (onsite or via Retrieval Services Queensland (RSQ)) for a child requiring more than two doses of Adrenaline IM or prior to administering Adrenaline IV.
Airway
- Children suffering from anaphylaxis who have respiratory distress without circulatory instability should be initially nursed in a sitting up position.
- Early preparation for advanced airway management
- For persistent stridor, consider nebulised adrenaline and continue to escalate anaphylaxis management Flowchart
Seek senior emergency/paediatric advice as per local practices for a child with airway concerns following administration of Adrenaline IM.
Contact the most senior resources available onsite (critical care/anaesthetic/ENT) prior to intubating a child with anaphylaxis.
Breathing
- high flow supplemental oxygen via non-rebreather mask is recommended
- for persistent wheeze, consider inhaled bronchodilators, magnesium, corticosteroids as per acute asthma management, in addition to escalating anaphylaxis management Flowchart
Circulation
- children with circulatory compromise should be nursed lying down
- elevate the lower extremities to conserve circulating volume
- IV access with two large-bore (age-appropriate) cannula, or intraosseous access, is recommended for children with severe symptoms at risk of circulatory compromise
- fluid resuscitation with sodium chloride 0.9% (in addition to IM adrenaline) for the management of shocked children
| Fluid resuscitation for the management of shocked children | |
|---|---|
| Bolus dose (IV or IO) |
Sodium Chloride 0.9% administered rapidly in 10 mL/kg bolus. Repeat in 10 mL/kg boluses as clinically indicated. |
- consideration of IV adrenaline infusion for refractory shock
- monitor for signs of overtreatment including pulmonary oedema and hypertension, with careful review and re-assessment of tachycardia, pallor and gastrointestinal symptoms
Seek urgent paediatric critical care advice (onsite or via RSQ) for a child in shock who is not responding to Adrenaline and fluids.'
Advanced Airway Management
Severe anaphylaxis is an incredibly challenging clinical scenario even for experienced clinicians. While most children respond well to IM adrenaline, airway swelling and bronchospasm can occur rapidly, with respiratory arrest being the cause of death in 86% fatal anaphylaxis cases.20
Preparation for early intubation with escalation to the most senior clinician available onsite is recommended if the child is desaturating. The airway should always be considered difficult, requiring smaller than usual endotracheal tube (ETT) size for age9. Caution should also be applied to Rapid Sequence Induction (RSI), requiring lower doses of sedation but maximising paralysis.
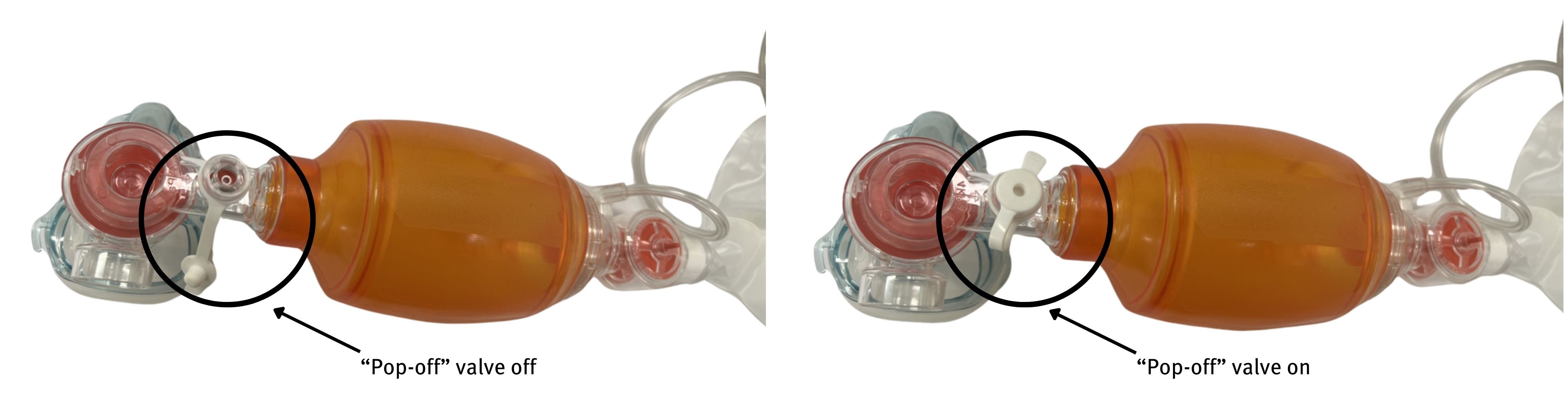
For the patient with progressive hypoxia or confusion despite maximum medical management, early intubation needs to be considered with anticipation of high airway pressure. When performing bag valve mask (BVM) ventilation, the pop off valve may need to be closed to achieve pressures required to overcome bronchospasm, while considering risk of inadvertent barotrauma.
Similarly, ventilation settings may need to be adjusted for peak inspiratory pressure (PIP) >50 and increased I:E, with consideration of pneumothorax in the case of secondary deterioration.
In the event intubation is unsuccessful, a clear escalation plan needs to be defined, with a surgical airway to be performed in the CICO situation.21
Profound and/or refractory anaphylaxis
Retrieval and admission to a paediatric critical care unit should be considered in any child with refractory anaphylaxis, any child with high risk or history of biphasic anaphylaxis, comorbidities such as asthma and for any patient with adrenaline infusion.
Anaphylactic shock displays features of both distributive and hypovolemic shock. If hypotension continues despite maximal adrenaline administration and large volume fluid resuscitation, additional therapies need to be considered and prepared22. These include additional vasopressors such as argipressin (vasopressin) (infusion via DERS software pumps at 0.01-0.12 unit/kg/h for < 20kg, 0.6-2.4unit/kg/hour for > 20kg) and methylene blue for profound vasodilatation (single dose 1 to 2 mg/kg by 20min infusion).
This should be discussed early with a senior physician in the paediatric intensive care unit or with the paediatric medical coordinator (PMC) via Retrieval Service Queensland (phone number 1300 799 127).
Adjuvant Therapy
IM adrenaline is the first-line treatment for anaphylaxis. Additional therapies only to be used in conjunction with escalating anaphylaxis management.
Nebulised adrenaline
- nebulised Adrenaline may help relieve upper airway obstruction (stridor)
| Adrenaline (NEB) dosing for the treatment of upper airway obstruction | |
|---|---|
| Dose | 5 mL of undiluted 1:1000 Adrenaline nebulised with oxygen as a single dose. Dose may be repeated in 10 minutes if there is inadequate response(1) See skill sheet Adrenaline use in Stridor |
Inhaled bronchodilators
- may help relieve bronchospasm if lower airway obstruction (wheeze) is a concern18
| Inhaled Salbutamol dosing to aide in the treatment of anaphylaxis in children | |
|---|---|
| Metered dose inhaler (MDI)* 100 micrograms (spacer recommended) | Age 1-5 years: 6 puffs Age 6 years or more: 12 puffs |
| Nebulised | Age 1-5 years: 2.5 mg Age 6 years or more: 5 mg |
| Continuous nebulised Salbutamol | Neat Salbutamol nebuliser solution (5 mg/mL), replenish where reservoir empty. Use 5 mg/1 mL nebules or 30 mL multi-use bottle. |
Corticosteroids
- not recommended unless there is a component of asthma aggravation with anaphylaxis, which should be treated concurrently as per the Asthma Guideline.
Corticosteroid dosing for the treatment of asthma exacerbations in anaphylaxis in children | |
|---|---|
| Prednisolone (oral) | Day 1: 2 mg/kg (maximum 50 mg) Day 2 and 3: 1 mg/kg |
| Dexamethasone (oral/IM/IV) | Single dose on day 1 of 0.6mg/kg (maximum 16mg)1 Dexamethasone 0.5mg and 4mg tablets are available but they are not easily dispersed in water to give in a partial dose. Doses that can be rounded to full tablet size can however be crushed and dispersed in water.28 Dexamethasone injection can be given orally and is tasteless. If IV stock is in shortage, please give liquid suspension. |
| Hydrocortisone (IV) | 4 mg/kg (maximum 100 mg) then every six hours on day one |
OR Methylprednisolone (IV) | 1 mg/kg (maximum 60 mg) then every six hours on day one |
While corticosteroids are commonly recommended as second-line treatment internationally, little evidence supports their use in anaphylaxis. No randomised controlled trials (in adults or children) were identified in a Cochrane Systematic Review of glucocorticoids for the treatment of anaphylaxis.15 The primary action of glucocorticoids is down-regulation of the late-phase eosinophilic inflammatory response, as opposed to the early-phase response. Short-term glucocorticoid treatment is seldom associated with adverse effects.16 The proposed rationale for corticosteroid administration is to prevent biphasic or protracted reactions.2 However, in two paediatric studies of biphasic reactions the administration of steroids did not appear to be preventative.2
Antihistamines
- not recommended in acute anaphylaxis as there is no evidence to support use17
Generalised and local allergic reaction
Antihistamines
- H1 antagonists are recommended to treat allergy symptoms including urticaria, angioedema and itchiness
- two-to-four-day-course taken orally is recommended to alleviate persistent symptoms after a severe allergic reaction
Sedating antihistamines including promethazine (Phenergan) or dexchlorpheniramine maleate (Polaramine) are NOT recommended as may cause significant side effects such as respiratory depression, especially in younger children.
Antihistamine dosing for the treatment of allergic reaction in children
| Antihistamine | Age | Dose |
|---|---|---|
| Cetirizine (Oral) (Zyrtec) | 1-2 years | 2.5 mg twice daily |
| 2-6 years | 5 mg once daily or 2.5 mg twice daily | |
| 6-12 years | 10 mg once daily or 5 mg twice daily | |
| 12-18 years | 10 mg once daily |
*Loratadine, Fexofenadine and Desloratadine are not available within QH Hospitals but are available in the community. Fexofenadine and Desloratadine can be prescribed to infants 6 months and over.
Escalation and advice outside of ED
Critically unwell or rapidly deteriorating child
| Includes children with the following (as a guide) | |||
|---|---|---|---|
| |||
| Less than 1 year | 1-4 years | 5-11 years | Over 12 years |
|
|
|
|
| Reason for contact | Who to contact |
|---|---|
| For immediate onsite assistance including airway management (anticipate difficult airway) | The most senior resources available onsite at the time as per local practices. Options may include:
|
| Paediatric critical care advice and assistance | Onsite or via Retrieval Services Queensland (RSQ). If no onsite paediatric critical care service contact RSQ on 1300 799 127:
RSQ (access via QH intranet) Notify early of child potentially requiring transfer. Consider early involvement of local paediatric/critical care service. In the event of retrieval, inform your local paediatric service. |
Non-critical child
| May include children with: |
|---|
|
| Reason for contact | Who to contact |
|---|---|
| Advice (including management, disposition or follow-up) | Follow local practices. Options:
|
| Referral | First point of call is the onsite/local paediatric service |
Inter-hospital transfers
| Do I need a critical transfer? |
|
| Request a non-critical inter-hospital transfer |
|
| Non-critical transfer forms |
|
Disposition
When to consider discharge from ED
Children with a localised or general allergic reaction
Children with a localised allergic reaction may be safely discharged.
Children with a general allergic reaction may be safely discharged provided symptoms have not progressed and are improving within one hour of observation.
On discharge
- parents / carers should be educated on allergic reactions and instructed to return immediately if symptoms recur
- Adrenaline autoinjectors must be prescribed (and if possible dispensed) to all children who have suffered any allergic reaction (mild, moderate or severe) secondary to nut exposure as subsequent exposures may lead to more severe reactions (including anaphylaxis) and are less predictable compared to other foods
Follow-up
- with GP within a week.
For children with a generalised allergic reaction, consider referral to a local Immunologist (via ED or GP) on discharge. Refer to the ASCIA website (https://allergy.org.au/) for registered local Immunologists. Refer to local Paediatrician if no local Immunology service.
Children with anaphylaxis
Consider discharge for children who meet the following criteria:
- resolution of respiratory and CVS symptoms
- an observation period of four hours following administration of Adrenaline IM.
Prior to discharge, consider other factors including the time of day, parents/carers comprehension and compliance, access to transport should return be required and distance to the local hospital.
On discharge
- caregivers must receive:
- two Adrenaline autoinjectors (AAI) (see table below). If dispensing from afterhours cupboard (in relevant hospitals) a non-PBS script can be provided for a single AAI and script a second AAI on PBS to take with the family. Make family aware of short expiry dates on AAI.
- education on how and when to administer the AAI (refer to How to give Epipen – Australasian Society of Clinical Immunology and Allergy (ASCIA)). And when to administer the AAI (refer to https://www.allergy.org.au/hp/anaphylaxis/first-aid-for-anaphylaxis).
- an individualised Action Plan (see Action Plan for Anaphylaxis on ASCIA website)
- general information regarding allergies and anaphylaxis management (see ASCIA website)
- the child and their caregiver/s should be encouraged to document the circumstances leading up to an episode of anaphylaxis (up to six to eight hours prior to symptoms)
| Age (years) | Weight of child | Adrenaline recommended on discharge |
|---|---|---|
| <1 | Less than 7.5 kg | Adrenaline ampoules are no longer recommended due to their risk of dosing error. Strict household allergen avoidance to nest the child is recommended. If there remains a significant risk and QAS would not be available to attend in a reasonable time, an Epipen® Jnr can be prescribed at the clinician discretion |
| 1-5 | 7.5-20 kg | Epipen® Jr and Anapen® Junior 150 autoinjector |
| 5-12 | Greater than 20 kg | Epipen® and Anapen® 300 autoinjector |
| >12 | Greater than 50 kg | Anapen® 500 autoinjector (or Epipen® 300 autoinjector at clinician discretion) |
Follow-up
- refer (via ED or GP) to Immunologist/Allergy specialist if available locally, otherwise refer to local Paediatrician
- if allergen known to be food related, consider referral to local dietician
When to consider admission
Facilities without a Short Stay Unit (SSU)
Admission is recommended for children with anaphylaxis who:
- have persistent symptoms four hours after treatment
- required more than two Adrenaline doses (due to possibility of recurrent symptoms)
Facilities with a Short Stay Unit (SSU)
Consider admission to a SSU for children who are responding to treatment but require a period of observation prior to meeting the criteria for discharge.
When to consider admission to inpatient ward from SSU
Admission to an inpatient service is recommended for children who require more than two Adrenaline doses (due to possibility of recurrent symptoms) or who are failing to improve after 12 hours of care.
- Australian Society of Clinical Immunology and Allergy (ASCIA). (2009), ASCIA Guidelines for adrenaline autoinjector prescription,] online] Available at: https://www.allergy.org.au [cited 2011 July 21].
- Santillanes, G., Davidson, J. (2010), ‘An evidence-based review of pediatric anaphylaxis’, Pediatric Emergency Medicine Practice, 7(10).
- de Silva, I.L., Mehr, S.S., Tey, D., et al. (2008), ‘Paediatric anaphylaxis: a 5-year retrospective review‘, Allergy. 63 (8): pp. 1071-1076.
- Thomson, H., Seith R., Craig, S. (2017) ‘Inaccurate diagnosis of paediatric anaphylaxis in three Australian Emergency Departments’, Journal of Paediatrics and Child Health, 53: pp 698-704.
- Queensland Health, Department of Emergency Medicine: Royal Children’s Hospital (Brisbane). (2008), Department of emergency medicine clinical guidelines, 7th Queensland Government: Brisbane (AU): p. 24
- Branganza, S.C., Acworth, J.P., Mckinnon, D.R., et al. (2006), ‘Paediatric emergency department anaphylaxis: Different patterns from adults’, Archives of Disease in Childhood, 91 (2): pp. 159-163.
- Mullins, R.J., Wainstein, B.K., Barnes, E.H., Liew, W.K., Campbell, D.E. (2016), ‘Increase in anaphylaxis fatalities in Australia from 1997 to 2013’, Clinical & Experimental Allergy, 46: pp. 1099-1110.
- Pumphrey, R. (2004), ‘Anaphylaxis: Can we tell who is at risk of a fatal reaction?’, Current Opinion in Allergy and Clinical Immunology. 4 (4): pp. 285-290.
- Davis, J. (2005), ‘Allergies and anaphylaxis: analysing the spectrum of clinical manifestations’, Emergency Medicine Practice, 7(10): pp. 1-23.
- Sheikh, A., Shehata, Y.A., Brown, S.G.A., et al. (2008), ‘Adrenaline (epinephrine) for the treatment of anaphylaxis with and without shock’, Cochrane Database of Systematic Reviews, Issue 4. Art. No.: CD006312.
- Simons, F.E.R., Roberts, J.R., Gu, X., et al. (1998), ‘Epinephrine absorption in children with a history of anaphylaxis’, Journal of Allergy and Clinical Immunology, 101 (1): pp. 33-37.
- Simons, F.E.R., Gu, X., Simons, K.J. (2001), ‘Epinephrine absorption in adults: Intramuscular versus subcutaneous injection’, Journal of Allergy and Clinical Immunology, 108 (5): pp. 871-873.
- Davis, J.E., Norris, R.L. (2007), ‘Allergic emergencies in children: The pivotal role of epinephrine’, Pediatric Emergency Medicine Practice, 4 (2).
- McLean-Tooke, A.P.C., Bethune, C.A., Fay, A.C., et al. (2003), ‘Adrenaline in the treatment of anaphylaxis: What is the evidence?’, British Medical Journal, 327 (7427): pp. 1332-1335.
- Choo, K.J.L., Simons, F.E.R., Sheikh, A. (2010), ‘Glucosteroids for the treatment of anaphylaxis (review)’, Cochrane Database of Systematic Reviews., Issue 3. Art. No.: CD007596.
- Schleimer, R.P. (2008), ‘Pharmacology of glucocorticoids in allergic disease’, in Middleton’s Allergy Principles and Practice, eds N.F. Adkinson, B.S. Bochnet, W.W. Busse, et al., 7th edn, Mosby:St Louis, pp. 1549-1574.
- Sheikh, A., ten Broek, V.M., Brown, S.G.A., et al. (2007), ‘H1-antihistamines for the treatment of anaphylaxis with and without shock’, Cochrane Database of Systematic Reviews, Issue 1. Art. No.: CD006160.
Document ID: CHQ-GDL-60011
Version number: 5.1
Supersedes: 5.0
Approval date: 15/08/2024
Effective date: 10/10/2024
Review date: 15/08/2028
Executive sponsor: Executive Director Medical Services
Author/custodian: Queensland Emergency Care Children Working Group
Applicable to: Queensland Health medical and nursing staff
Document source: Internal (QHEPS) + External
Authorisation: Executive Director Clinical Services QCH
Keywords: Allergy, anaphylaxis, acute allergic reaction, Paediatric, emergency, guideline, children, 60011
Accreditation references: NSQHS Standards (1-8): 1 Clinical Governance, 4 Medication Safety, 8 Recognising and Responding to Acute Deterioration
This guideline is intended as a guide and provided for information purposes only. View full disclaimer.